Clinical data under EU MDR: why you have more options than you might think
When manufacturers hear 'clinical evaluation', many instinctively think 'clinical investigation'. But under the EU MDR, that is just one possibility for clinical data collection among many.
If you’re exploring Article 61(10), it’s time to widen your lens: clinical performance data can come from more than just clinical trials.
Clinical evaluation ≠ Clinical investigation
EU Medical Device Regulation (MDR) requires that manufacturers demonstrate compliance with General Safety and Performance Requirements (GSPRs). But how you generate data to illustrate this is actually quite flexible.
Clinical data, as defined in Article 2(51) of the EU MDR, includes evidence from:
- Clinical investigations (yes, the traditional route)
- Published literature on the device in question, or on equivalent devices
- Clinical experience (including from post-market surveillance)
- Retrospective datasets, curated registries, and other real-world sources
This variety opens the door to strategic decisions. Think of it like a box of chocolates: not all data sources will suit your device, but more are available than you may have considered.
The three domains of clinical data
To align with medical-device-software-specific guidance, you must provide clinical data across three domains:
- Technical performance — Do the technical characteristics of the device reliably, accurately, and consistently fulfil its intended purpose in real-world usage?
- Clinical association — Is there a logical and scientifically supported link between the device’s output and the targeted clinical condition?
- Clinical performance — Are the clinical benefits achieved when the device is used as intended?
For more details on these data types needed for clinical evaluation, refer to our previous blog on this topic.
Curating a robust clinical evaluation requires coverage of these three domains, as well as determining how to acquire the right data for each. Evidence can be identified from existing sources, such as published literature or real-world registries, or can be generated through new studies, validation testing, or prospective trials. The balance between identification and generation will vary by domain, the novelty of the device, and the strength of the existing evidence.
Let's have a look at the options available for identifying and generating data for each domain:
Clinical association data
Clinical association data is used to demonstrate the link between the device’s measurements or functions and the targeted medical condition or situations.
Identification:
- Literature from similar devices and the generally acknowledged clinical state of the art
Generation:
- Prospective clinical studies when the association is novel or not well established
- Real-world evidence when existing data is lacking
Technical performance data
Technical performance data is used to assess whether the device provides reliable and consistent outputs when provided with the intended input of data. Typically data for the technical performance of a device will be generated during verification and validation activities, however it may be possible to leverage data from an equivalent/legacy device from the same manufacturer.
Identification:
- Technical performance from an equivalent/legacy device from the same manufacturer
Generation:
- Software validation and verification testing
- Bench testing, simulation studies, cadaver or phantom models
- Algorithm validation and robustness testing
- Verification and validation testing of generalisability using historic data
Clinical performance data
Clinical performance data is used to confirm that the device performs safely and effectively in the intended clinical environment.
Identification:
- Literature evidence of clinical performance and safety from equivalent devices
Generation:
- Prospective clinical investigations
- Usability testing for human factors
- Post-market clinical follow-up studies
When is new clinical data necessary?
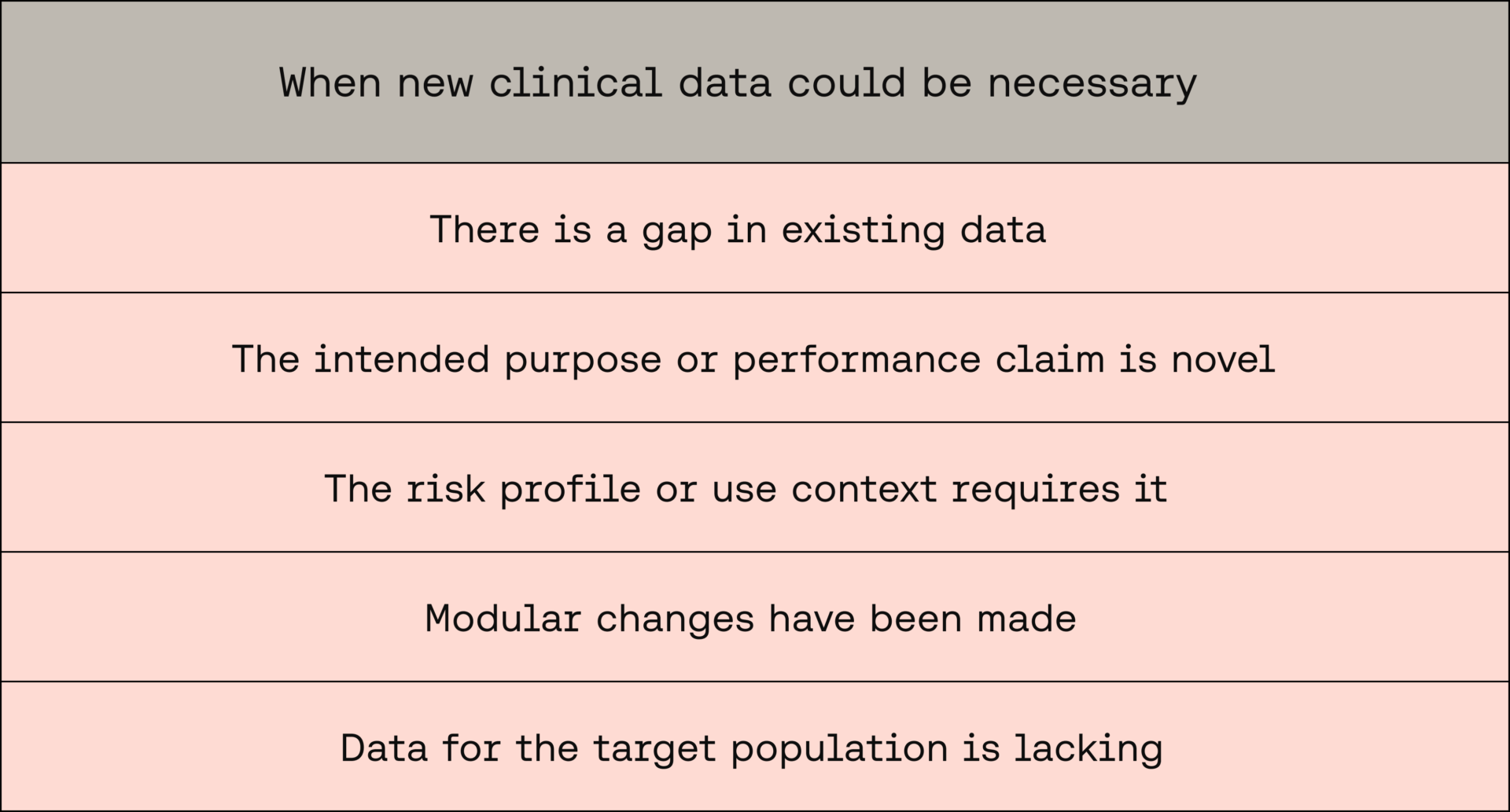
MDCG 2020-1 emphasises that generating new clinical data may be required when:
1. There is a gap in existing data
Gap analyses should be performed to determine if existing data (e.g. from literature or similar devices) is insufficient to demonstrate:
- Valid clinical association
- Technical performance
- Clinical performance
“VALID CLINICAL ASSOCIATION / SCIENTIFIC VALIDITY may further be demonstrated by the creation of new CLINICAL PERFORMANCE DATA in the cases where existing data is not sufficient.”
2. The intended purpose or performance claim is novel
New data may be needed to support the clinical benefit and safety profile if the device includes:
3. The risk profile or use context requires it
For example:
- When the output impacts patient-management decisions
- When direct diagnostic or therapeutic effects are claimed
- When software predicts a future clinical state (e.g. prognosis, risk scores)
“If the MDSW is used for the determination of a patient’s future state... or if the output impacts clinical outcomes... a prospective study may be required.”
4. Modular changes have been made
- New releases or modified modules may require performance validation for just the changed modules, if independent
- If changes affect the intended use or combination of features, the entire final configuration may need to be re-evaluated
“Validation of the CLINICAL PERFORMANCE should be considered at each change of the software to a new release.”
5. Data for the target population is lacking
Retrospective analyses may be used if they are:
- Derived from the target population
- Of sufficient amount and quality
- Ethically and legally compliant
If not, prospective studies may be necessary.
“Such an approach is only possible under condition that there is an adequate access to data sets of sufficient amount and quality and obtained from the target population.”
Mapping your data-collection strategy
To promote a proactive and expansive data-collection strategy, ask yourself:
- What do I already have?
- Literature? Retrospective data? Equivalent device data?
- Is it enough?
-
- Is the data relevant, high-quality, and from your target population?
- Where are the gaps?
-
- And what relevant data can you collect to fill them?
Where to go from here: Build a proactive clinical evaluation process
Now that you understand the full menu of data options and ways to collect relevant clinical and technical data, it’s time to build a strategy that’s not just a one-off plan, but a sustainable process tailored to your device.
Start by identifying what data you currently have available, including from external sources (e.g. literature searches), and what data you may need to collect prior to your submission. This helps to promote a systematic, evidence-based, clinical evaluation.
A key output of this process is your Clinical Evaluation Plan (CEP) that:
- Documents the intended purpose and claims
- Lists the data sources used to address each performance domain
- Maps any gaps and outlines how they will be addressed
- Aligns with PMCF plans where needed
Tip: Document not only what you plan to do, but why that pathway is justified based on existing evidence and risk.
Approaching clinical evaluation as an ongoing, multi-source, evidence-driven strategy, rather than a cost-intensive hurdle centred on clinical investigations, will better equip you to justify your technical documentation, address evidence gaps, and help demonstrate your device’s safety and performance under MDR requirements.
Want Scarlet news in your inbox?
Sign up to receive updates from Scarlet, including our newsletter containing blog posts, sent straight to you by email.